According to ergonomic definition, a Repetitive Strain Injury or RSI is an injury to a part of the body caused by overusing or straining that body part. The body gets strained when the body parts are put to hard work, stretched farther, put to greater impact, directly or otherwise, and are made to function at a level higher than it is prepared for. The immediate impact may be minor, but when it occurs repeatedly, the constant straining becomes a cause for damage. The term ‘Repetitive Strain Injury’ identifies a group of conditions that result from using the body in a way it is not designed for or capable of comfortable working. Repetitive Strain Injuries also have been described as painful and limiting soft tissue failures that result from repeated or continuous application of slight to moderate physical stress over extended period of time.
Other terms that are used interchangeably with Repetitive Stress Injury are Repetitive Stress Disorder (RSD), Repetitive Strain Disorder (RSD), Repetitive Motion Injury (RMI), Repetitive Motion Disorder (RMD) and Cumulative Trauma Disorder (CTD). Another term ‘Musculoskeletal Disorders (MSDs)’, to be more specific, a Work-related Musculoskeletal Disorder (WMSD), refers not only to conditions that involve the nerves, tendons, muscles, and supporting structures of the body, but is also used interchangeably with RSI.
Many workplace factors influence repetitive motion problems which lead to strain, and thus injury. The three main factors that cause strain injuries due to repetitive motion (also called Repetitive Strain Injuries or RSI) are Force, Repetition and Posture. Force is the pressure exerted or encountered; Repetitions are related to cycle time; and Postures concern the position of the body while performing a given operation. Other factors that lead to strains and injuries are inadequate training, incentives given to work for longer hours, change in method or product model and physical condition of the worker such as pregnancy, menopause and hysterectomy. Acceleration is emerging as an additional workplace factor, specially related to the upper extremities.
Forces and Repetitions
Forces and repetitions are two interrelated factors. A force is considered low when average adjusted force (mean + variance) = 6.6 pounds +/- 3.52 pounds. An average adjusted force (mean + variance) of 27.94 pounds +/- 18.92 is considered as high force.
A task is considered repetitive if the cycle time is less than 30 seconds and the task is performed for more than 50% of the work shift.
One of the revolutionary researches by Tom Armstrong shows that cases of Repetitive Strain Injury in low force and low repetition operations are rare while that of high force and high repetition are maximum.
However, it is important to understand two important factors that determine the risk of Repetitive Strain Injury (RSI) in workers’ operations: firstly, the number of times the forces are exerted during the course of the work day; and secondly, the position of the body part which exerts or encounters the force.
The National Institute for Occupational Safety and Health (NIOSH), USA document established the epidemiologic evidence of the relationship between selected RSI of the upper extremity and the low back and exposure to physical factors at work. The Bureau of Labour Statistics (BLS) of the US Department of Labour reported in 1990 that of all the reported cases of occupational illness, 56% were associated with repeated strain injuries. The body parts affected were shoulder (6%), wrist (51%), hand – excluding fingers (6%), and other body parts (37%). In 1997, the NIOSH reported that about 7,00,000 cases (or 32%) were the result of repetitive motion or overexertion. It also reported that RSIs accounted for 14% of physician visits and 19% of hospital stays.
Hazardous Body Postures
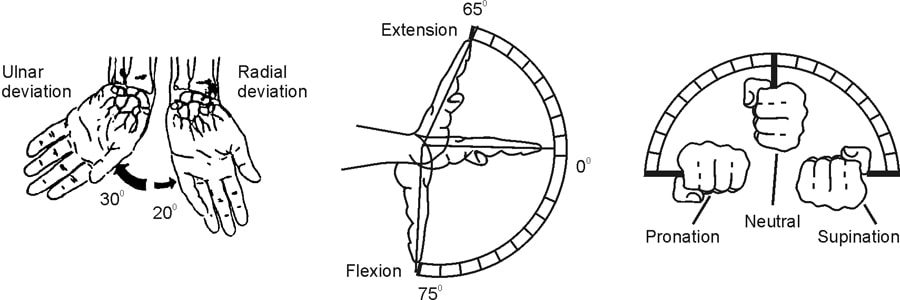
Wrist
Extremes of ulnar deviation; Extremes of radial deviation
This represents the movement of wrist towards little finger or thumb. It is advisable not to exceed the extremes, of 300 for ulnar and 200 for radial deviation.
Extremes of wrist flexion; Extremes of wrist extension
“Wrist should remain straight,” this is the ideal position for wrist. The extension should not be more than 650 whereas flexion should not exceed 750.
Extremes of wrist supination; Extremes of wrist pronation
Wrist should remain as close to neutral as possible during much of the work cycle as possible. Pronation and supination at about 900 can give harmful effects.
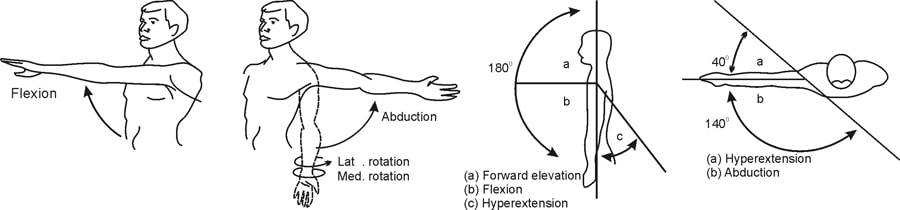
Shoulder
Shoulder flexion
Shoulder flexion should not exceed 900. It pertains to movement of hand from shoulder point towards front.
Shoulder abduction and rotation
Shoulder abduction should not exceed 180-200. Abduction reflects movement of hand from shoulder point towards lateral side. Greater than 50-100 of medial or lateral shoulder rotation along with 150-200 of shoulder abduction can cause traumas.
Hyperextension of shoulder
Hyperextension is extension of abduction towards back. It should not exceed 400.
Other body parts
FINGERS — Lumbrical and pinch grasps
Pinch grip involves lifting of items with the help of thumb and one finger only, whereas lumbrical grasp is a fatiguing posture for the small muscles of the hand, causing ache of the palm. This is a posture where the fingers are straight except the thumb and grasp is done by the thumb.
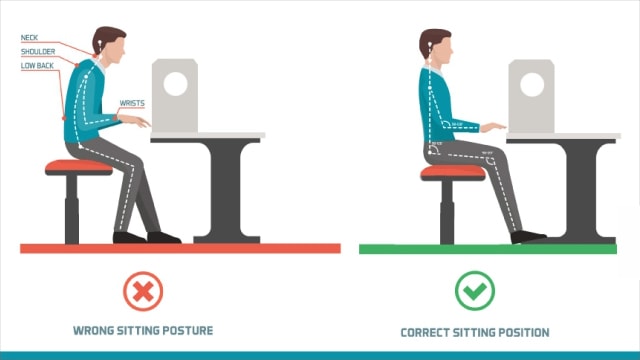
NECK — Greater than 200 of neck flexion
Neck should not be more than 200 flexion from its normal position.
LOWER BACK
Leaning or bending of lower back beyond 18” for females, 22” for males is a hazardous posture.
Postures
No clear definition of ‘posture’ can be found in ergonomics literature. It may be regarded as the configuration of the body’s head, trunk and limbs in space or as a quasi-static bio-mechanical alignment, depending on whether the particular context in which it is used is anatomical or bio-mechanical. In any work situation, functional, geometric and bio-mechanical aspects are as integral to the concept of posture as they are to the consequences for performance and comfort.
Pilot study data of laboratory experiment supports the hypothesis that extreme or complex postures correlate negatively with task performance. Sewing machine separation task can be characterized by “low force exertion, but with high speed manipulation, frequent repetition of hand movement and long duration of continuous work under a constrained body posture”. An awkward sitting posture can be influenced by the interaction of several factors, including work place layout (e.g. seat and table height and inclination), task location (task height, distance and direction), and manual and/or visual requirements of the tasks and the anthropometric characteristics of the seated worker. The tendency of operators to work in the hunched posture suggests a potential conflict between workstation geometry and operator dimension. Analyses indicate that most commonly operators position the chair away from the work surface in order to allow a knee angle of 1,100 or greater. Factors limiting operator access to the workstation were the location of the treadle, which is too close to the proximal edge and various obstructions (motors, pneumatic equipment and machine guards) beneath the work surface. While typical recommended knee room averages of about 46 cm, the presence of these obstructions, in some cases, limit available space to less than 26 cm.
An increase in task distance and increase in trunk forward flexion, results in decrease in head/neck flexion. As the task height moves downwards relative to subject’s horizontal eye level, there is an increase in (move forward bending) head-neck flexion but decrease in trunk forward flexion (more upright posture). This suggests that a comfortable visual distance is needed in order to see the task position even for a normal task which is not visually demanding. Task is located within the distance of 50-70 cm and at a height of about 20 cm, below horizontal eye level which appears ideal.
Repetitive Strain Injuries and Disorders
Exposure to repetitive, forceful or awkward tasks over a period of time result in stressful situations which most often result in micro-traumas to a specific region of the body, such as a muscle or tendon. Without adequate recovery, the accumulation of micro-traumas results in pain, discomfort, numbness, reduced strength and/or inhibited dexterity.
Examples of injuries or disorders that can be work-related include:
Carpal Tunnel Syndrome (CTS) — It is a medical condition in which the median nerve is compressed at the wrist, leading to paresthesia, numbness and muscle weakness in the hand.
Tendonitis (or Tendinitis) — It is an inflammation of a tendon. In this disorder, the tendons become inflamed for a variety of reasons, and the action of pulling the muscle becomes irritating. For example, patellar tendonitis, also known as the jumper’s knee, is an inflammation of the patellar tendon, which connects the tibia to the patella.
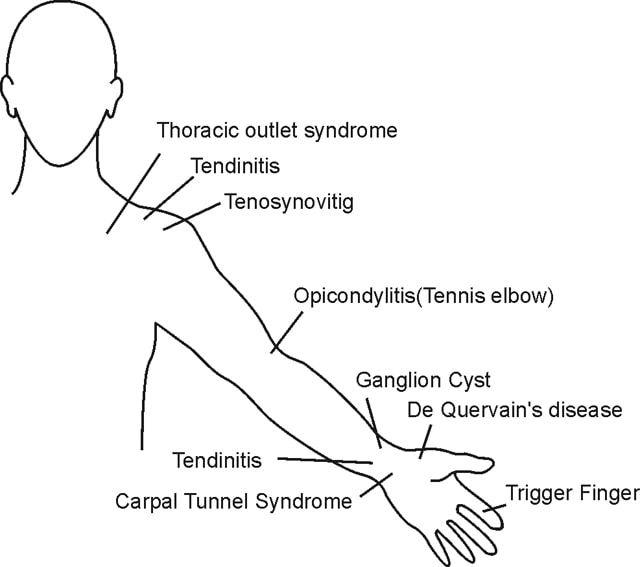
Tenosynovitis — It is the inflammation of the fluid-filled sheath (called the synovium) that surrounds a tendon. Symptoms of tenosynovitis include pain, swelling and difficulty moving the particular joint where the inflammation occurs.
Rotator Cuff Syndrome — The rotator cuff is a band of tendons which compose a portion of the shoulder joint. Rotator cuff syndrome is suggested by shoulder pain when the arm is elevated to the side. A rotator cuff tear, particularly if severe, will make it difficult or impossible to maintain the arm lifted up to 900.
De Quervain’s Disease — An inflammable or a tendinosis of the sheath or tunnel that surrounds two tendons which control movement of the thumb.
Trigger Finger — Sometimes tenosynovitis (discussed earlier) causes the finger to “stick” in a flexed position; this is called “stenosing” tenosynovitis, as commonly called “Trigger Finger”.
Tarsal Tunnel Syndrome — Tarsal tunnel syndrome is a compression, or squeezing on specific nerve that lies on the inside of the ankle, next to the ankle bones. It produces symptoms anywhere along the path of the nerve. Tarsal tunnel syndrome is similar to carpal tunnel syndrome, which occurs in the wrist. Both disorders arise from the compression of a nerve in a confined space. It is a cause of foot and ankle pain in adults.
Sciatica — The sciatic nerve is the longest nerve in a human body. It runs from the spinal cord to the buttock and hip area and down the back of each leg. The term “sciatica” refers to pain that radiates along the path of this nerve – from the back down the buttock and leg.
Epicondylitis — Epicondyle is the outside (lateral side) of the elbow. Epicondylitis refers to an inflammation of an epicondyle. It is of two types:
Lateral epicondylitis, also known as tennis elbow — A condition where the outer part of the elbow becomes painful and tender. It’s a condition that is commonly associated with playing tennis (or cricket, in Sachin Tendulkar’s case), though the injury can happen to almost anybody.
Medial epicondylitis, also known as golfer’s elbow — Pain and inflammation on the inner side of the elbow, where the tendons of forearm muscles attach to the bony bump on the inside of elbow. The pain may spread into forearm and wrist. It’s not limited to golfers. Tennis players and others who repeatedly use their wrists or clench their fingers also can develop golfer’s elbow.
Raynaud’s Phenomenon — A condition resulting in a particular series of discolorations of the fingers and/or the toes after exposure to changes in temperature (cold or hot) or emotional events.
Carpet Layers Knee — Abnormalities in the soft tissue of the anterior part of the knee, caused by protracted mechanical stress.
Herniated Spinal Disc — The spinal disc is a soft cushion that sits between each vertebrae of the spine. This spinal disc becomes more rigid with age. In a young individual, the disc is soft and elastic, but like so many other structures in the body, the disc gradually loses its elasticity and is more vulnerable to injury. As the spinal disc becomes less elastic, it can rupture. When the disc ruptures, a portion of the spinal disc pushes outside its normal boundary – this is called a herniated disc. Common symptoms of a herniated disc include Electric Shock Pain, Tingling & Numbness, Muscle Weakness and Bowel or Bladder Problems.
Low back pain — This refers to pain in the lumbosacral area of the spine encompassing the distance from the 1st lumbar vertebra to the 1st sacral vertebra. This is the area of the spine where the lordotic curve forms. The most frequent site of low back pain is in the 4th and 5th lumbar segment.
| Tasks | High Forces | High Repetitions | Extreme Postures | Low Back | Shoulder | Wrist | Hand | Thumb | Fingers | ||||||||
| L | R | L | R | L | R | L | R | L | R | L | R | L | R | L | R | ||
| Side Seam | X | X(1320) | X | X | X | X | X | X | X | ||||||||
| Loading | X(6900) | X | X | X | Pinch | X | X | ||||||||||
| Hem Pant Legs | X(1260) | X | X | X | X | X | X | X | X | ||||||||
| Sew Buttons of Cuffs | X4800-6000 | X | X | X | X | X | X | Pinch | Pinch | ||||||||
| Buttoning | X | X(4800)L | X | X | X | X | X | ||||||||||
| Thread Clipping | X | X(2700) | X | X | |||||||||||||
| Folding | X | (1400-2160) Pins Only | X | X | X | X | X | X | |||||||||
| Side Body | X (1424) | X | X | X | X | X | X | ||||||||||
| Basting | X | X(9840) | X | X | X | X | X | X | X | ||||||||
| Bag Pockets | X | X | X (3105) | X | X | X | X | X | X | X | X | X | |||||
| Waistband | X | X | X ( 6120) | X | X | X | X | X | X | X | X | X | X | X | |||
| Source: AAMA Manual | |||||||||||||||||
Epidemiologic Study: Detection of repetitive strain injuries
The goal of epidemiologic studies is to identify factors that are associated (positively or negatively) with the development or recurrence of adverse medical conditions. This evaluation and summary of the epidemiologic evidence focuses chiefly on disorders that affect the neck and the upper extremity, including tension neck syndrome, shoulder tendinitis, epicondylitis, carpal tunnel syndrome and hand-arm vibration syndrome, which have been the most extensively studied in the epidemiologic literature. The relationship between workplace factors and the development of RSIs from epidemiologic studies is classified into one of the following categories:
Strong evidence of work-relatedness (+++)
A causal relationship is shown to be very likely between intense or long duration exposure to the specific risk factor(s) and RSI when the epidemiologic criteria of causality are used. A positive relationship has been observed between exposure to the specific risk factor and Repetitive Strain Injury in studies in which chance, bias and confounding factors could be ruled out with reasonable confidence in at least several studies.
Evidence of work-relatedness (++)
Some convincing epidemiologic evidence show a causal relationship when the epidemiologic criteria of causality for intense or long duration exposure to the specific risk factor(s) and Repetitive Strain Injury are used. A positive relationship has been observed between exposure to the specific risk factor and Repetitive Strain Injury in studies in which chance, bias and confounding factors are not the likely explanation.
| Repetition | Force | Posture | Combination | Vibration | |
|---|---|---|---|---|---|
| NECK and NECK / SHOULDER | ++ | ++ | +++ | +/0 | |
| SHOULDER | ++ | +/0 | ++ | +/0 | |
| ELBOW | +/0 | ++ | +/0 | +++ | |
| HAND / WRIST (Carpal tunnel syndrome) | ++ | ++ | +/0 | +++ | ++ |
| HAND / WRIST (Tendinitis) | ++ | ++ | ++ | +++ | |
| HAND-ARM vibration syndrome | +++ | ||||
| BACK | +++ | ++ | +++ |
Insufficient evidence of work-relatedness (+/0)
The available studies are of insufficient number, quality, consistency or statistical power to permit a conclusion regarding the presence or absence of a causal association. Some studies suggest a relationship to specific risk factors but chance, bias or confounding may explain the association.
Evidence of no effect of work factors (-)
Adequate studies consistently show that the specific workplace risk factor(s) are not related to development of Repetitive Strain Injury.
It is clear from the below table that combination of factors rather any single factor poses more risk of Repetitive Strain Injury.
Despite many years of research/efforts, the occupational exposure limits of different risk factors for development of RSIs have not yet been established. One of the problems in setting such guidelines is the limited understanding of how different risk factors of RSIs interact in causing the injury. It is unfortunate that in most sewing operations, the excursions of arm and hand movements are too much to allow elbow support. Further the sewing operators use highly repetitive movements which often require a holding action of muscles. The steady holding actions or sustained postures result in static loading and fatigue. Highly repetitive tasks do not allow adequate time for muscles to rest. Recovery time can occur with job rotation. A carefully planned job rotation schedule may ensure use of different muscles and thus recovery time for muscles significantly reduce risk of RSI. Apart from job rotation engineered workstation layout, height adjustability of workstations and specialty tools are several other ways to minimize the risk of RSI.





